
What is Asthma?

Introduction :
Asthma is a chronic disease characterized by recurrent attacks of breathlessness and wheezing, which vary in severity and frequency from person to person.

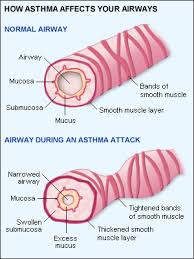
Asthma symptoms start when allergens or other irritants cause the lining of the airways to swell (become inflamed) and narrow. The muscles around the airways can then spasm, (contract rapidly), causing the airways to narrow even more. When the lining of the airways is inflamed, it produces more mucus. The mucus clogs the airways and further blocks the flow of air. This is called an "asthma attack."
Classification :
Asthma is clinically classified according to the frequency of symptoms, FEV1 and peak expiratory flow rate.


Clinical classification of asthma severity | ||||
Severity | Symptom frequency | Nighttime symptoms | Peak expiratory flow rate or FEV1 of predicted | Variability of peak expiratory flow rate or FEV1 |
Intermittent | Less than once a week | Less than twice per month | More than 80% predicted | Less than 20% |
Mild persistent | More than once per week but less than once per day | More than twice per month | More than 80% predicted | 20–30% |
Moderate persistent | Daily | More than once per week | 60–80% predicted | More than 30% |
Severe persistent | Daily | Frequent | Less than 60% predicted | More than 30% |
Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic), based on whether symptoms are precipitated by allergens (atopic) or not (non-atopic).
Signs & Symptoms :
Severity of asthma attack | ||||
Sign/Symptom | Mild | Moderate | Severe | Pending arrest |
Alertness | May show agitation | Agitated | Agitated | Confused/Drowsy |
Breathlessness | On walking | On talking | Even at rest | |
Talks in | Sentences | Phrases | Words | |
Wheeze | Moderate | Loud | Loud | Absent |
Accessory muscle | Usually not used | Used | Used | |
Respiratory rate (/min) | Increased | Increased | Often >30 | |
Pulse rate (/min) | 100 | 100-120 | >120 | <60> |
PaO2 | >60 | <60>cyanosis | ||
PaCO2 | <45 | <45 | >45 | |
Cause :

Asthma is caused by environmental and genetic factors, which can influence how severe asthma is and how well it responds to medication. Some environmental and genetic factors have been confirmed by further research, while others have not been. Underlying both environmental and genetic factors is the role of the upper airway in recognizing the perceived dangers and protecting the more vulnerable lungs by shutting down the airway. Profet has argued that allergens look to our immune systems like significant threats. Asthma, in this view, is seen as an evolutionary defense.

Environmental :
Many environmental risk factors have been associated with asthma development and morbidity in children, but a few stand out as well-replicated or that have ameta-analysis of several studies to support their direct association.
Environmental tobacco smoke, especially maternal cigarette smoking, is associated with high risk of asthma prevalence and asthma morbidity, wheeze, and respiratory infections.Low air quality, from traffic pollution or highozone levels, has been repeatedly associated with increased asthma morbidityand has a suggested association with asthma development that needs further research.
Recent studies show a relationship between exposure to air pollutants (e.g. from traffic) and childhood asthma. This research finds that both the occurrence of the disease and exacerbation of childhood asthma are affected by outdoor air pollutants.
Caesarean sections have been associated with asthma when compared with vaginal birth; a meta-analysis found a 20% increase in asthma prevalence in children delivered by Caesarean section compared to those who were not. It was proposed that this is due to modified bacterial exposure during Caesarean section compared with vaginal birth, which modifies the immune system (as described by the hygiene hypothesis).
Psychological stress has long been suspected of being an asthma trigger, but only in recent decades has convincing scientific evidence substantiated this hypothesis. Rather than stress directly causing the asthma symptoms, it is thought that stress modulates the immune system to increase the magnitude of the airway inflammatory response to allergens and irritants.
Viral respiratory infections at an early age, along with siblings and day care exposure, may be protective against asthma, although there have been controversial results, and this protection may depend on genetic context.
Antibiotic use early in life has been linked to development of asthma in several examples; it is thought that antibiotics make one susceptible to development of asthma because they modify gut flora, and thus the immune system (as described by the hygiene hypothesis). The hygiene hypothesis is a hypothesisabout the cause of asthma and other allergic disease, and is supported by epidemiologic data for asthma. For example, asthma prevalence has been increasing in developed countries along with increased use of antibiotics, c-sections, and cleaning products. All of these things may negatively affect exposure to beneficial bacteria and other immune system modulators that are important during development, and thus may cause increased risk for asthma and allergy.
Recently scientists connected the rise inprevalence of asthma, to the rise in use ofparacetamol, suggesting the possibility that paracetamol can cause asthma.
It has been suggested that viral infections such as HSV and CSV are correlated to asthma episodes.
Genetic :
Over 100 genes have been associated with asthma in at least one genetic association study. However, such studies must be repeated to ensure the findings are not due to chance.
Many of these genes are related to the immune system or to modulating inflammation. However, even among this list of highly replicated genes associated with asthma, the results have not been consistent among all of the populations that have been tested. This indicates that these genes are not associated with asthma under every condition, and that researchers need to do further investigation to figure out the complex interactions that cause asthma. One theory is that asthma is a collection of several diseases, and that genes might have a role in only subsets of asthma. For example, one group of genetic differences (single nucleotide polymorphisms in17q21) was associated with asthma that develops in childhood.
Gene–environment interactions :
Research suggests that some genetic variants may only cause asthma when they are combined with specific environmental exposures, and otherwise may not be risk factors for asthma.
The genetic trait, CD14 single nucleotide polymorphism(SNP) C-159T and exposure toendotoxin (a bacterial product) are a well-replicated example of a gene-environment interaction that is associated with asthma. Endotoxin exposure varies from person to person and can come from several environmental sources, including environmental tobacco smoke, dogs, and farms. Researchers have found that risk for asthma changes based on a person’sgenotype at CD14 C-159T and level of endotoxin exposure.
CD14-endotoxin interaction based on CD14 SNP C-159T | ||
Endotoxin levels | CC genotype | TT genotype |
High exposure | Low risk | High risk |
Low exposure | High risk | Low risk |
Pathophysiology :
Bronchoconstriction :

During an asthma episode, inflamed airways react to environmental triggers such as smoke, dust, or pollen. The airways narrow and produce excess mucus, making it difficult to breathe. In essence, asthma is the result of an immune response in the bronchialairway.

The airways of asthma patients are "hypersensitive" to certain triggers, also known asstimuli (see below). (It is usually classified astype I hypersensitivity.) In response to exposure to these triggers, the bronchi(large airways) contract intospasm (an "asthma attack").Inflammation soon follows, leading to a further narrowing of the airways and excessive mucus production, which leads to coughing and other breathing difficulties. Bronchospasm may resolve spontaneously in 1–2 hours, or in about 50% of subjects, may become part of a 'late' response, where this initial insult is followed 3–12 hours later with further bronchoconstriction and inflammation.
The normal caliber of the bronchus is maintained by a balanced functioning of these systems, which both operate reflexively. Theparasympathetic reflex loop consists of afferent nerve endings which originate under the inner lining of the bronchus. Whenever these afferent nerve endings are stimulated (for example, by dust, cold air or fumes) impulses travel to the brain-stem vagal center, then down the vagal efferent pathway to again reach the bronchial small . Acetylcholine is released from the efferent nerve endings. This acetylcholine results in the excessive formation of inositol 1,4,5-trisphosphate (IP3) in bronchial smooth muscle cells which leads to muscle shortening and this initiates bronchoconstriction.


Bronchial inflammation :
The mechanisms behind allergic asthma—i.e., asthma resulting from an immune response to inhaled allergens—are the best understood of the causal factors. In both people with asthma and people who are free of the disease, inhaled allergens that find their way to the inner airways areingested by a type of cell known asantigen-presenting cells, or APCs. APCs then "present" pieces of the allergen to other immune systemcells. In most people, these other immune cells (TH0 cells) "check" and usually ignore the allergen molecules. In asthma patients, however, these cells transform into a different type of cell (TH2), for reasons that are not well understood.
The resultant TH2 cells activate an important arm of the immune system, known as thehumoral immune system. The humoral immune system produces antibodiesagainst the inhaled allergen. Later, when a patient inhales the same allergen, these antibodies "recognize" it and activate ahumoral response. Inflammation results: chemicals are produced that cause the wall of the airway to thicken, cells which produce scarring to proliferate and contribute to further 'airway remodeling', causes mucus producing cells to grow larger and produce more and thicker mucus, and the cell-mediated arm of the immune system is activated. Inflamed airways are more hyper-reactive, and will be more prone to bronchospasm.
The "hygiene hypothesis" postulates that an imbalance in the regulation of these THcell types in early life leads to a long-term domination of the cells involved in allergic responses over those involved in fighting infection. The suggestion is that for a child being exposed to microbes early in life, taking fewer antibiotics, living in a large family, and growing up in the country stimulate the TH1 response and reduce the odds of developing asthma.
Stimuli :
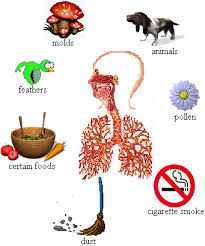
§ Allergens from nature, typically inhaled, which include waste from common household pests, the house dust mite and cockroach, as well asgrass pollen,moldspores, and petepithelial cells;
§ Indoor air pollution fromvolatile organic compounds, including perfumes and perfumed products. Examples include soap, dishwashing liquid, laundry detergent, fabric softener, paper tissues, paper towels, toilet paper, shampoo, hairspray, hair gel, cosmetics, facial cream, sun cream, deodorant, cologne, shaving cream, aftershave lotion, air freshener and candles, and products such as oil-based paint.
§ Medications, includingaspirin, β-adrenergic antagonists (beta blockers), and penicillin.
§ Food allergies such as milk,peanuts, and eggs. However, asthma is rarely the only symptom, and not all people with food or other allergies have asthma
§ Sulfite sensitivity Asthma can occur in reaction to ingestion or inhalation of sulfites, which are added to foods and wine as preservatives.
§ Salicylate sensitivitySalicylates can trigger asthma in sensitive individuals. Salicylates occur naturally in many healthy foods. Aspirin is also a salicylate.
§ Use of fossil fuel relatedallergenic air pollution, such as ozone, smog, summer smog,nitrogen dioxide, andsulfur dioxide, which is thought to be one of the major reasons for the high prevalence of asthma inurban areas.
§ Various industrial compounds (e.g. toluene diisocyanate) and other chemicals, notablysulfites;chlorinated swimming pools generatechloramines—monochloramine (NH2Cl), dichloramine (NHCl2) and trichloramine (NCl3)—in the air around them, which are known to induce asthma.
§ Early childhood infections, especially viral upper respiratory tract infections. Children who suffer from frequent respiratory infections prior to the age of six are at higher risk of developing asthma,particularly if they have a parent with the condition. However, persons of any age can have asthma triggered by colds and other respiratory infections even though their normal stimuli might be from another category (e.g. pollen) and absent at the time of infection. In many cases, significant asthma may not even occur until the respiratory infection is in its waning stage, and the person is seemingly improving. In children, the most common triggers are viral illnesses such as those that cause the common cold.
§ Exercise or intense use of respiratory system—the effects of which differ somewhat from those of the other triggers, since they are brief. They are thought to be primarily in response to the exposure of the airway epithelium to cold, dry air.
§ Hormonal changes inadolescent girls and adult women associated with theirmenstrual cycle can lead to a worsening of asthma. Some women also experience a worsening of their asthma duringpregnancy whereas others find no significant changes, and in other women their asthma improves during their pregnancy.
§ Psychological stress. There is growing evidence that psychological stress is a trigger. It can modulate the immune system, causing an increased inflammatory response to allergens and pollutants.
§ Cold weather can make it harder for patients to breathe. Whether high altitude helps or worsens asthma is debatable and may vary from person to person.
Pathogenesis :
The fundamental problem in asthma appears to beimmunological: young children in the early stages of asthma show signs of excessive inflammation in their airways.Epidemiological findings give clues as to thepathogenesis: the incidence of asthma seems to be increasing worldwide, and asthma is now very much more common in affluent countries.
In 1968 Andor Szentivanyifirst described The Beta Adrenergic Theory of Asthma; in which blockage of the Beta-2 receptors of pulmonary smooth muscle cells causes asthma. Szentivanyi's Beta Adrenergic Theory is a citation classic[94] using theScience Citation Index and has been cited more times than any other article in the history of theJournal of Allergy and Clinical Immunology.
In 1995 Szentivanyi and colleagues demonstrated that IgE blocks beta-2 receptors.Since overproduction of IgE is central to all atopic diseases, this was a watershed moment in the world of allergy.
Asthma and sleep apnea :
It is recognized with increasing frequency that patients who have bothobstructive sleep apnea and asthma often improve tremendously when the sleep apnea is diagnosed and treated. CPAP is not effective in patients with nocturnal asthma only.
Asthma and gastro-esophageal reflux disease :
If gastro-esophageal reflux disease (GERD) is present, the patient may have repetitive episodes of acid aspiration. GERD may be common in difficult-to-control asthma, but according to one study, treating it does not seem to affect the asthma.When there is a clinical suspicion for GERD as the cause of the asthma, anEsophageal pH Monitoring is required to confirm the diagnosis and establish the relationship between GERD and asthma.
Risk factors :
Risk factors :
Studying the prevalence of asthma and related diseases such as eczema and hay feverhave yielded important clues about some key risk factors. The strongest risk factor for developing asthma is a family history of atopic disease; this increases one's risk of hay fever by up to 5x and the risk of asthma by 3-4x. In children between the ages of 3-14, a positive skin test for allergies and an increase in immunoglobulin Eincreases the chance of having asthma. In adults, the more allergens one reacts positively to in a skin test, the higher the odds of having asthma.
Because much allergic asthma is associated with sensitivity to indoor allergens and because Western styles of housing favor greater exposure to indoor allergens, much attention has focused on increased exposure to these allergens in infancy and early childhood as a primary cause of the rise in asthma. Primary prevention studies aimed at the aggressive reduction of airborne allergens in a home with infants have shown mixed findings. Strict reduction of dust mite allergens, for example, reduces the risk of allergic sensitization to dust mites, and modestly reduces the risk of developing asthma up until the age of 8 years old.However, studies also showed that the effects of exposure to cat and dog allergens worked in the converse fashion; exposure during the first year of life was found to reduce the risk of allergic sensitization and of developing asthma later in life.
The inconsistency of this data has inspired research into other facets of Western society and their impact upon the prevalence of asthma. One subject that appears to show a strong correlation is the development of asthma and obesity. In the
Hygiene hypothesis :
One theory for the cause of the increase in asthma prevalence worldwide is the so-called "hygiene hypothesis"—that the rise in the prevalence of allergies and asthma is a direct and unintended result of the success of modern hygienic practices in preventing childhood infections. Studies have shown repeatedly that children coming from environments one would expect to be less hygienic (East Germany vs. West Germany,families with many children, day care environments) tended to have lower incidences of asthma and allergic diseases. This seems to run counter to the logic that viruses are often causative agents in exacerbation of asthma.Additionally, other studies have shown that viral infections of the lower airway may in some cases induceasthma, as a history ofbronchiolitis or croup in early childhood is a predictor of asthma risk in later life.Studies which show that upper respiratory tract infections are protective against asthma risk also tend to show that lower respiratory tract infections conversely tend to increase the risk of asthma.
Population disparities :
Asthma prevalence in the
Asthma prevalence also differs populations of the same ethnicity who are born and live in different places.US-born Mexican populations, for example, have higher asthma rates than non-US born Mexican populations that are living in the
Asthma prevalence and asthma deaths also differ by gender. Males are more likely to be diagnosed with asthma as children, but asthma is more likely to persist into adulthood in females. Women account for nearly 65% of all asthma related deaths. This difference may be attributable to hormonaldifferences, among other things. In support of this, girls who reach puberty before age 12 were found to have a later diagnosis of asthma more than twice as much as girls who reach puberty after age 12. Asthma is also the number one cause of missed days from school.
Socioeconomic factors :

The incidence of asthma is highest among low-income populations (asthma deaths are most common in low to middle income countries), which in the western world are disproportionately ethnic minorities and are more likely to live near industrial areas. Additionally, asthma has been strongly associated with the presence ofcockroaches in living quarters, which is more likely in such neighborhoods.
Asthma incidence and quality of treatment varies among different racial groups, though this may be due to correlations with income (and thus affordability of health care) and geography. For example, African Americans are less likely to receive outpatient treatment for asthma despite having a higher prevalence of the disease. They are much more likely to have emergency room visits or hospitalization for asthma, and are three times as likely to die from an asthma attack compared to whites. The prevalence of "severe persistent" asthma is also greater in low-income communities compared with communities with better access to treatment. It is important that parents, most especially of those families with relatively low socioeconomic status are educated and informed of all necessary information about asthma since their family, particularly their children are vulnerable to persistent asthma. For this reason, more health organizations participate in the move for education and information as fight against asthma.
Asthma and athletics :
Asthma appears to be more prevalent in athletes than in the general population. One survey of participants in the 1996 Summer Olympic Games, in
There appears to be a relatively high incidence of asthma in sports such ascycling, mountain biking, and long-distance running, and a relatively lower incidence in weightlifting and diving. It is unclear how much of these disparities are from the effects of training in the sport.
Occupational asthma :
Asthma as a result of (or worsened by) workplace exposures is the world's most commonly reported occupational respiratory disease. Still most cases of occupational asthma are not reported or are not recognized as such. Estimates by the American Thoracic Society (2004) suggest that 15–23% of new-onset asthma cases in adults are work related. In one study monitoring workplace asthma by occupation, the highest percentage of cases occurred among operators,fabricators, and laborers(32.9%), followed by managerial and professional specialists (20.2%), and in technical, sales, and administrative support jobs (19.2%). Most cases were associated with themanufacturing(41.4%) andservices (34.2%) industries. Animal proteins,enzymes, flour, natural rubberlatex, and certain reactive chemicals are commonly associated with work-related asthma. When recognized,
these hazards can be mitigated, dropping the risk of disease.
Diagnosis :
Asthma is defined simply as reversible airway obstruction. Reversibility occurs either spontaneously or with treatment. The basic measurement is peak flow rates and the following diagnostic criteria are used by the British Thoracic Society:
§ ≥20% difference on at least three days in a week for at least two weeks;
§ ≥20% improvement of peak flow following treatment, for example:
§ 10 minutes of inhaled β-agonist (e.g., salbutamol);
§ six weeks of inhaledcorticosteroid (e.g.,beclometasone);
§ 14 days of 30 mgprednisolone.
§ ≥20% decrease in peak flow following exposure to a trigger (e.g., exercise).
In many cases, a physician can diagnose asthma on the basis of typical findings in a patient's clinical history and examination. Asthma is strongly suspected if a patient suffers from eczemaor other allergic conditions—suggesting a general atopic constitution—or has a family history of asthma. While measurement of airway function is possible for adults, most new cases are diagnosed in children who are unable to perform such tests.
In children, the key to asthma diagnosis is the sound of wheezing or a high-pitched sound upon exhalation. Other clues are recurrent wheezing, breathing difficulty, or chest tightness, or a history of coughing that is worse at night. The doctor should also know if the child's symptoms are worse with exercise, colds,or exposure to certain irritants such as smoke, emotional stress, or changes in the weather.
Other information important to diagnosis is the age at which symptoms began and how they progressed, the timing and pattern of wheezing, when and how often a child had to visit a clinic or hospital emergency department because of symptoms, whether the child ever tookbronchodilatormedication for the symptoms and the nature of the response to medication.
Although pediatricians may tend to ask parents for information about their children's symptoms, studies suggest that children themselves are reliable sources as early as age 7 and perhaps even as early as age 6.
In adults and older children, diagnosis can be made withspirometry or a peak flow meter(which tests airway restriction), looking at both the diurnal variation and any reversibility inhaledbronchodilator medication. The latest guidelines from the
The NAEPP guidelines do not recommend testing peak expiratory flow as a regular screening method, because it is more variable than spirometry. However, testing peak flow at rest (or baseline) and after exercise can be helpful, especially in young patients who may experience only exercise-induced asthma. It may also be useful for daily self-monitoring and for checking the effects of new medications. Peak flow readings can be charted ongraph paper charts together with a record of symptoms or use peak flow charting software. This allows patients to track their peak flow readings and pass information back to their doctor or nurse.
In the Emergency Department, doctors may use a capnography which measures the amount of exhaled carbon dioxide,along with pulse oximetrywhich shows the percentage of hemoglobin that is carrying oxygen, to determine the severity of an asthma attack as well as the response to treatment.
More recently, exhaled nitric oxide has been studied as abreath test indicative of airway inflammation in asthma.
Differential Diagnosis :
Before diagnosing someone as having asthma, alternative possibilities should be considered. A clinician taking a history should check whether the patient is using any known bronchoconstrictors (substances that cause narrowing of the airways, e.g. certainanti-inflammatoryagents orbeta-blockers). Among elderly patients, the presenting symptom may be fatigue, cough, or difficulty breathing, all of which may be erroneously attributed toCOPD, congestive heart failure, or simple aging.
After a pulmonary function test has been carried out, radiological tests, such as achest X-ray or CT scan, may be required to exclude the possibility of other lung diseases. Occasionally, abronchial challenge test may be performed usingmethacholine orhistamine to assessbronchial hyperresponsiveness.
Chronic obstructive pulmonary disease, is a syndrome which closely resembles asthma, is correlated with more exposure to cigarette smoke, an older patient, less symptom reversibility after bronchodilator administration (as measured by spirometry), and decreased likelihood of family history of atopy. Most people found to have the syndrome are subsequently found to have asthma and many diagnosed asthmatics go on to develop the syndrome.
Pulmonary aspiration, whether direct due todysphagia (swallowing disorder) or indirect (due to acid reflux), can show similar symptoms to asthma. However, with aspiration, fevers might also indicateaspiration pneumonia. Direct aspiration (dysphagia) can be diagnosed by performing a Modified Barium Swallow test and treated with feeding therapy by a qualified speech therapist. If the aspiration is indirect (from acid reflux) then treatment directed at this is indicated.
In some people, asthma-like symptoms may be triggered by gastroesophageal reflux disease, which can be treated with suitable antacids.
A majority of children who are asthma sufferers have an identifiable allergy trigger. Specifically, in a 2004 study, 71% had positive test results for more than 1 allergen, and 42% had positive test results for more than 3 allergens.
The majority of these triggers can often be identified from the history; for instance, patients with hay fever orpollen allergy will have seasonal symptoms, those with allergies to pets may experience an abatement of symptoms when away from home, and those withoccupational asthma may improve during leave from work. Allergy tests can help identify some avoidable symptom triggers.
Asthma is categorized by theUnited States National Heart, Lung, and Blood Institute as falling into one of four categories: intermittent, mild persistent, moderate persistent and severe persistent. The diagnosis of "severe persistent asthma" occurs when symptoms are continual with frequent exacerbations and frequent night-time symptoms, result in limited physical activity and when lung function as measured by PEV or FEV1tests is less than 60% predicted with PEF variability greater than 30%.
Prevention and control :
Prevention of the development of asthma is different from prevention of asthma episodes. Aggressive treatment of mild allergy withimmunotherapy has been shown to reduce the likelihood of asthma development. In controlling symptoms, the crucial first step intreatment is for patient and doctor to collaborate in establishing a specific plan of action to prevent episodes of asthma by avoiding triggers and allergens, regularly testing for lung function, and using preventive medications (see especially "Control of Environmental Factors"
Current treatment protocols recommend controller medications such as an inhaledcorticosteroid, which helps to suppressinflammation and reduces the swelling of the lining of the airways, in anyone who has frequent (greater than twice a week) need of relievers or who has severe symptoms. If symptoms persist, additional controller drugs are added until almost all asthma symptoms are prevented. With the proper use of control drugs, patients with asthma can avoid the complications that result from overuse of rescue medications.
Patients with asthma sometimes stop taking their controller medication when they feel fine and have no problems breathing. This often results in further attacks after a time, and no long-term improvement.
The only preventive agent known is allergen immunotherapy. Controller medications include the following:
§ Inhaled glucocorticoids are the most widely used prevention medications and normally come as inhaler devices (ciclesonide,beclomethasone,budesonide,flunisolide,fluticasone,mometasone, andtriamcinolone). Long-term use of corticosteroids can have many side effects including a redistribution of fat, increased appetite, bloodglucose problems and weight gain. High doses of steroids may causeosteoporosis. These side effects are generally not seen with the inhaled steroids when used in conventional doses for control of asthma due to the smaller dose which is targeted to the lungs, unlike the higher doses of oral or injected preparations. Patients on the highest doses of inhaled steroids should take prophylactic treatment (usually Calcium and exercise, but sometimes Fosamax or similar) to prevent osteoporosis. Deposition of steroids in the mouth may result in oral thrush. Deposition near the vocal cords can cause hoarse voice. These may be minimised by rinsing the mouth with water after inhaler use, as well as by using a spacer. Spacers also generally increase the amount of drug that reaches the lungs. A new agent, ciclesonide, is inactive until activated in the lung. For this reason changing to ciclesonide can relieve dysphonia in some patients. In November 2007 The New York Times reported a review of more than 500 studies finding that independently backed studies on inhaled corticosteroids are up to four times more likely to find adverse effects than studies paid for by drug companies.
§ Leukotriene modifiers (montelukast, zafirlukast,pranlukast, and zileuton) provide both anti-spasm and anti-inflammatory effects. In general they are weaker than inhaled corticosteroids, but the do not have any steroid side-effects and the benefit is additive with inhaled steroid.
§ Mast cell stabilizers (cromoglicate (cromolyn), and nedocromil). These medications are believed to prevent the initiation of the allergy reaction, by stabilizing the mast cell. They are not effective once the reaction has already begun, and typically must be used 4 times a day for maximal effect. But they do truly prevent asthma symptoms and are nearly free of side-effects.
§Antimuscarinics/anticholinergics (ipratropium, oxitropium, and tiotropium). These agents both relieve spasm and reduce formation of mucous. They are more effective in patients with empysema or 'smokers lung.' They are rarely effective in asthma and are not true asthma controller medications.
§ Methylxanthines (theophylline andaminophylline). These agents are bronchodilators with minimal anti-inflammatory effect. At one time they were the only effective asthma medications available. They are sometimes considered if sufficient control cannot be achieved with inhaled glucocorticoid, leukotriene modifier, and long-acting β-agonist combinations.
§ Antihistamines are often used to treat the nasal allergies which can accompany asthma. Older agents are too drying and can result in thick mucous so should be avoided. Newer antihistamines which do not have this effect can safely be used by patients with asthma.
§ Allergy Desensitization, also known as allergy immunotherapy, may be recommended in some cases where allergy is the suspected cause or trigger of asthma. Allergy shots are dangerous in severe asthma and in uncontrolled asthma. However if allergy immunotherapy is started early in the disease there is a good chance that a remission of asthma can be induced (aka "asthma cure"). Typically the need for medication is reduced by about half with injection allergy immunotherapy, when done correctly. If a patient is only allergic to one or two items, oral allergy immunotherapy can be used. This is safe, much easier in young children, and is about half as effective. Unfortunately if a patient is allergic to more than 2 or 3 items then oral therapy cannot be given in a dose which is proven safe and effective.
§ Omalizumab, an IgEblocker, can help patients with severe allergic asthma that is not well controlled with other drugs. It is expensive, but not compared with hospitalization(s). It requires regular injections.
§ Methotrexate is occasionally used in some difficult-to-treat patients.
§ If chronic acid indigestion (GERD) contributes to a patient's asthma, it should also be treated, because it may prolong the respiratory problem.
§ Chronic sinus disease may be a contributing factor in difficult to control asthma, and should be evaluated.
Trigger avoidance :
As is common with respiratory disease, smokingis believed to adversely affect patients in several ways, including an increased severity of symptoms (likely due to increased inflammation), a more rapid decline of lung function, and decreased response to preventive medications.Automobile emissions are considered an even more significant cause and aggravating factor. Patients with asthma who smoke or who live near traffictypically require additional medications to help control their disease. Furthermore, exposure of both non-smokers and smokerssecond-hand smoke is detrimental, resulting in more severe asthma, moreemergency room visits, and more asthma-related hospital admissions, but the effect of woodstove and gas stove fumes is uncertain. Smoking cessation and avoidance of second-hand smoke is strongly encouraged in people who have asthma. Air filters and room air cleaners may help prevent some asthma symptoms.Ozone is also considered as a major factor in increasing asthma.The report by the National Heart, Lung and Blood Institute[3] supports the idea of an asthma management plan that includes the avoidance of as many allergens as possible to which the individual is sensitive. This report, and others also agree that no one single approach is sufficient to reduce allergens; a multifactorial approach is required. The Asthma and Allergy FriendlyCertification Program that is operated in the USA by the Asthma and Allergy Foundation of America and in Canada by the Asthma Society of Canada is based on this multifactorial approach to trigger control.
For those in whom exercise can trigger an asthma attack (exercise-induced asthma), higher levels of ventilation and cold, dry air tend to exacerbate attacks. For this reason, activities in which a patient breathes large amounts of cold air, such as skiing and running, tend to be worse for people with asthma, whereas swimming in an indoor, heated pool with warm, humid air is less likely to provoke a response.
Diet & Supplements :
Beverages that contain caffeine provide a slight amount of bronchodilation for an hour or two, but taking a rescue inhaler is much more effective for the temporary relief of asthma symptoms.
Low intake of vitamin C has been linked to pulmonary dysfunction and several studies have shown that increasing vitamin C intake may improve lung function in people with asthma and provide a protective effect against exercise-induced asthma. Ascorbic acid supplementation attenuates exercise-induced bronchoconstriction in patients with asthma. While results have been positive, it is unlikely that vitamin C alone will attenuate the effects of asthma. Larger and methodologically stronger studies are necessary before vitamin C can be recommended for people with asthma.
Treatment :
Perhaps the most important step in controlling asthma is establishing a partnership between doctor and patient (whether child or adult) to create a specific, customized plan for proactively monitoring and managing symptoms. It is essential to be certain that someone who has asthma understands (and takes an active part in deciding) what needs to be accomplished, including reducing exposure to allergens, taking medical tests to assess the severity of symptoms, and possibly using medications. The treatment plan should be written down, consulted at every visit, and adjusted according to changes in symptoms.


The most effective treatment for asthma is identifying triggers, such as pets or aspirin, and limiting or eliminating exposure to them. If trigger avoidance is insufficient, medical treatment is available.Desensitization has been suggested as a possible cure.Additionally, some trial subjects were able to remove their symptoms by retraining their breathing habits with the Buteyko method.
Other forms of treatment include relief medication, prevention medication, long-acting β2-agonists, and emergency treatment.
The specific medical treatment recommended to patients with asthma depends on the severity of their illness and the frequency of their symptoms. Specific treatments for asthma are broadly classified as relievers, preventers and emergency treatment. TheExpert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma(EPR-2)of the
The Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthmaof the U.S. National Asthma Education and Prevention Program, released in 2007, presented a focused 6-step approach to asthma management, based on four principles that act as a blueprint to guide individualized treatment:
§ Frequent and regular assessment of symptoms
§ Patient education
§ Control of environmental
§ Systematic evaluation of the effectiveness and safety of medications.
The 2007 revised NAEPP guidelines differ from the earlier version in an increased focus on asthma control and individualized treatment, reorganizing the goals of treatment to differentiate risk from impairment. They specify defined measures that should prompt a decision to "step up" or "step down" the intensity of treatment, and they emphasize education and integrated decision-making to encourage patient self-management.
Bronchodilators are recommended for short-term relief in all patients. For those who experience occasional attacks, no other medication is needed. For those with mild persistent disease (more than two attacks a week), low-dose inhaled glucocorticoids or alternatively, an oral leukotriene modifier, a mast-cell stabilizer, or theophylline may be administered. For those who suffer daily attacks, a higher dose of glucocorticoid in conjunction with a long-acting inhaled β-2 agonist may be prescribed; alternatively, a leukotriene modifier or theophylline may substitute for the β-2 agonist. In severe asthma, oral glucocorticoids may be added to these treatments during severe attacks.
Pharmaceutical agents :
Symptomatic control of episodes of wheezing and shortness of breath is generally achieved with fast-acting bronchodilators. These are typically provided in pocket-sized, metered-dose inhalers (MDIs). In young sufferers, who may have difficulty with the coordination necessary to use inhalers, or those with a poor ability to hold their breath for 10 seconds after inhaler use (generally the elderly), an asthma spacer(see top image) is used. The spacer is a plastic cylinder that mixes the medication with air in a simple tube, making it easier for patients to receive a full dose of the drug and allows for the active agent to be dispersed into smaller, more fully inhaled bits.

Chemical Name | Brand Name |
Almeterol
| Proventil HFA
|
A nebulizer which provides a larger, continuous dose can also be used. Nebulizers work by vaporizing a dose of medication in a saline solution into a steady stream of foggy vapour, which the patient inhales continuously until the full dosage is administered. There is no clear evidence, however, that they are more effective than inhalers used with a spacer. Nebulizers may be helpful to some patients experiencing a severe attack. Such patients may not be able to inhale deeply, so regular inhalers may not deliver medication deeply into the lungs, even on repeated attempts. Since a nebulizer delivers the medication continuously, it is thought that the first few inhalations may relax the airways enough to allow the following inhalations to draw in more medication.
Relievers include:
§ Short-acting, selectivebeta2-adrenoceptor agonists, such assalbutamol (albuterolUSAN),levalbuterol, terbutaline andbitolterol.
Tremors, the major side effect, have been greatly reduced by inhaled delivery, which allows the drug to target the lungs specifically; oral and injected medications are delivered throughout the body. There may also be cardiac side effects at higher doses (due to Beta-1 agonist activity), such as elevated heart rate or blood pressure. However, levalbuterol has been shown to have less cardiac side effects and significantly more anti-inflammatory effects on bronchial smooth muscle than its racemic counterpart albuterol. The question becomes does this justify its 5-10 fold higher cost. Some hospitals start a patient on levalbuterol until symptoms wane and then switch to albuterol. Patients must be cautioned against using these medicines too frequently, as with such use their efficacy may decline, producingdesensitizationresulting in an exacerbation of symptoms which may lead to refractory asthma and death.
§ Older, less selectiveadrenergic agonists, such as inhaled epinephrine andephedrinetablets, have also been used. Cardiac side effects occur with these agents at either similar or lesser rates to albuterol.When used solely as a relief medication, inhaled epinephrine has been shown to be an effective agent to terminate an acute asthmatic exacerbation. In emergencies, these drugs were sometimes administered by injection. Their use via injection has declined due to related adverse effects.
§ Anticholinergicmedications, such asipratropium bromide may be used instead. They have no cardiac side effects and thus can be used in patients with heart disease; however, they take up to an hour to achieve their full effect and are not as powerful as the β2-adrenoreceptor agonists.
§ Inhaled glucocorticoids are usually considered preventive medications while oral glucocorticoids are often used to supplement treatment of a severe attack. They should be used twice daily in children with mild to moderate persistent asthma.Arandomized controlled trialhas demonstrated the benefit of 250 microgbeclomethasonewhen taken as an as-needed combination inhaler with 100 microg ofalbuterol.
Long-acting β2-agonists
A typical inhaler, of Serevent (salmeterol), a long-acting bronchodilator.
Long-acting bronchodilators (LABD) are similar in structure to short-acting selective beta2-adrenoceptor agonists, but have much longer side chains resulting in a 12-hour effect, and are used to give a smoothed symptomatic relief (used morning and night). While patients report improved symptom control, these drugs do not replace the need for routine preventers, and their slow onset means the short-acting dilators may still be required. In November 2005, the American FDAreleased a health advisory alerting the public to findings that show the use of long-acting β2-agonists could lead to a worsening of symptoms, and in some cases death. In December 2008, members of the FDA's drug-safety office recommended withdrawing approval for these medications in children. Discussion is ongoing about their use in adults.
Currently available long-acting beta2-adrenoceptor agonists includesalmeterol,formoterol,bambuterol, and sustained-release oral albuterol. Combinations of inhaled steroids and long-acting bronchodilators are becoming more widespread; the most common combination currently in use is fluticasone/salmeterol (Advair in the
A recent meta-analysis of the roles of long-acting beta-agonists may indicate a danger to asthma patients. The study, published in the Annals of Internal Medicine in 2006, found that long-acting beta-agonists increased the risk for asthma hospitalizations and asthma deaths 2- to 4-fold, compared with placebo. "These agents can improve symptoms through bronchodilation at the same time as increasing underlying inflammation and bronchial hyper-responsiveness, thus worsening asthma control without any warning of increased symptoms," said Shelley Salpeter in a press release after the publication of the study. The release goes on to say that "Three common asthma inhalers containing the drugs salmeterol or formoterol may be causing four out of five
"Salpeter and colleagues also assert that salmeterol may be responsible for 4000 of the 5000 asthma-related deaths that occur in the
Dr. Shelley Salpeter, in a letter to the Annals of Internal Medicine, responds to the comments of Dr. Nelson, as follows:
"It is true that the asthma death rate increased after salmeterol was introduced, then peaked and is now starting to decline despite continued use of the long-acting beta-agonists. This trend in death rates can best be explained by examining the ratio of beta-agonist use to inhaled corticosteroids... In the recent past, inhaled corticosteroid use has increased steadily while long-acting beta-agonist use has begun to stabilize and short-acting beta-agonist use has declined... Using this estimate, we can imagine that if long-acting beta-agonists were withdrawn from the market while maintaining high inhaled corticosteroid use, the death rate in the
Acute exacerbation :
Acute exacerbation of asthma is generally referred to as an acute asthmatic attack. When an acute asthma attack is present, symptoms are quite dramatic and this is an emergent condition. In an instant, the individual can have breathing difficulties and even lose consciousness.
When an asthma attack is unresponsive to a patient's usual medication, other treatment options available for emergency management include:
§ Oxygen to alleviate thehypoxia that results from extreme asthma attacks (but not the asthma attack itself).
§ Nebulized salbutamol orterbutaline (short-acting beta-2-agonists), often combined with ipratropium (an anticholinergic).
§ Systemic steroids, oral or intravenous (prednisone,prednisolone,methylprednisolone,dexamethasone, orhydrocortisone). Some research has looked into an alternative inhaled route. A non tapered 5 - 10 day course seems to be sufficient.
§ Other bronchodilators that are occasionally effective when the usual drugs fail:
§ Intravenous salbutamol
§ Nonspecific beta-agonists, injected or inhaled (epinephrine,isoetharine,isoproterenol,metaproterenol)
§ Anticholinergics, IV or nebulized, with systemic effects (glycopyrrolate,atropine,ipratropium)
§ Methylxanthines (theophylline,aminophylline)
§ Inhalation anesthetics that have a bronchodilatory effect (isoflurane,halothane,enflurane)
§ The dissociative anaesthetic ketamine, often used inendotracheal tubeinduction
§ Magnesium sulfate, intravenous
§ Intubation andmechanical ventilation, for patients in or approaching respiratory arrest.
§ Heliox, a mixture of helium and oxygen, may be used in a hospital setting. It has a more laminar flow than ambient air and moves more easily through constricted airways.
Acute asthma exacerbation causes :
Some individuals will have stable asthma for weeks or months and then suddenly develop an episode of acute asthma. Different asthmatic individuals react differently to various factors. However, most individuals can develop severe exacerbation of asthma from several triggering agents.
Home factors that can lead to exacerbation includedust, house mites, animaldander (especially cat and dog hair), cockroach allergensandmolds at any given home. Perfumes are a common cause of acute attacks in females and children. Both virus and bacterial infections of the upper respiratory tract infection can worsen asthma.
Complementary medicine :
Many asthma patients, like those who suffer from other chronic disorders, usealternative treatments; surveys show that roughly 50% of asthma patients use some form of unconventional therapy.There is little data to support the effectiveness of most of these therapies. However, the Buteyko method of controlling hyperventilation hypocapnia has shown in five randomized controlled trials to result in a significant reduction in need for medications without an effect on bronchial hyperreactivity or lung function. In May 2008 the updated British Guidelines for the Management of Asthma endorsed Buteyko Technique. ACochranesystematic review of acupuncture for asthma found no evidence of efficacy. A similar review of air ionisers found no evidence that they improve asthma symptoms or benefit lung function; this applied equally to positive and negative ion generators.Another systematic study reviewed a range of dust mite control measures, including air filtration, chemicals to kill mites, vacuuming, mattress covers and others. Overall these methods had no effect on asthma symptoms. A study of "manual therapies" for asthma, includingosteopathic,chiropractic,physiotherapeutic andrespiratory therapeuticmanoeuvres, found there is insufficient evidence to support or refute their use in treating asthma;these manoeuvers include various osteopathic and chiropractic techniques to "increase movement in the rib cage and the spine to try and improve the working of the lungs and circulation"; chest tapping, shaking, vibration, and the use of "postures to help shift and cough up phlegm." Onemeta-analysis finds thathomeopathy may have a potentially mild benefit in reducing the intensity of symptoms. However, the number of patients involved in the analysis was small, and subsequent studies have not supported this finding.Several small trials have suggested some benefit from various yogapractices, ranging from integrated yoga programs,yogasanas, Pranayama,meditation, and kriyas, toSahaja yoga, a form of 'new religious' meditation.
Prognosis :
The prognosis for asthma is good, especially for children with mild disease.Of asthma diagnosed during childhood, 54% of cases will no longer carry the diagnosis after a decade. The extent of permanent lung damage in people with asthma is unclear. Airway remodelling is observed, but it is unknown whether these represent harmful or beneficial changes.Although conclusions from studies are mixed, most studies show that early treatment with glucocorticoids prevents or ameliorates decline in lung function as measured by several parameters. For those who continue to suffer from mild symptoms, corticosteroids can help most to live their lives with few disabilities.It is more likely to consider immediate medication of inhaled corticosteroids as soon as asthma attacks occur. According to studies conducted, patients with relatively mild asthma who have received inhaled corticosteroids within 12 months of their first asthma symptoms achieved good functional control of asthma after 10 years of individualized therapy as compared to patients who received this medication after 2 years (or more) from their first attacks. Though they (delayed) also had good functional control of asthma,they were observed to exhibited slightly less optimal disease control and more signs of airway inflammation.
The mortality rate for asthma is low, with around 6,000 deaths per year in a population of some 10 million patients in the
0 comments:
Post a Comment